Overview
The advent of high-resolution computed tomography (CT) scanning in the 1980s revolutionized diagnostic imaging of the temporal bone. CT scanning offers the greatest structural definition of any currently available imaging modality. [1, 2] The purpose of this article is to familiarize the reader with the normal anatomy of the temporal bone depicted by CT scanning. The article reviews the anatomy of the middle ear space and surrounding bone and presents radiographic imaging in both axial and coronal views, with labeled salient features and relevant text.
An axial view through the superior portion of the temporal bone can be seen below.
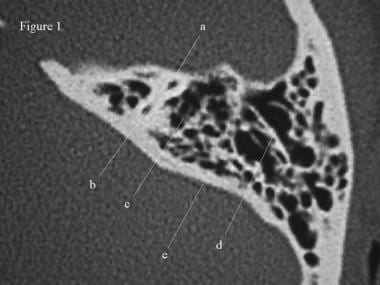 CT scan, temporal bone. An axial view through the superior portion of the temporal bone, which demonstrates the anterior (a) and posterior (b) crura of the superior semicircular canal. The surrounding otic capsule is observed as dense white bone. The mastoid air cells (c) are lateral to the otic capsule. The squamous air cells are separated from the petrous air cells by the Koerner septum (d). The posterior margin of the temporal bone, or cerebellar plate, (e) forms the anterior margin of the posterior cranial fossa.
CT scan, temporal bone. An axial view through the superior portion of the temporal bone, which demonstrates the anterior (a) and posterior (b) crura of the superior semicircular canal. The surrounding otic capsule is observed as dense white bone. The mastoid air cells (c) are lateral to the otic capsule. The squamous air cells are separated from the petrous air cells by the Koerner septum (d). The posterior margin of the temporal bone, or cerebellar plate, (e) forms the anterior margin of the posterior cranial fossa.
A study by Visvanathan and Morrissey used high-resolution CT scanning to determine that temporal bone variations are not uncommon. Evaluating 339 temporal bones, the investigators found that the incidences of deep sinus tympani, anteriorly located sigmoid sinus, high dehiscent jugular bulb, enlarged internal auditory meatus, and enlarged cochlear aqueduct were 5.01%, 2.94%, 2.76%, 1.76%, and 0.58%, respectively. [3]
A study by Shamshad et al using high-resolution CT scanning found pneumatization of the temporal bone to be more prevalent around the temporal mandibular joint (TMJ). Pneumatization prevalences were as follows [4] :
-
Peritubal area - 56%
-
Roof of the TMJ fossa - 52%
-
Articular eminence - 12%
-
Root of the zygomatic process - 5%
A CT-scan study by Takahashi et al found that different regions of the temporal bone mature at different ages, determining that the otic capsule demonstrates mature bone at birth, while the ages of maturation for the lateral surface of the mastoid cavity, the posterior cranial fossa, and the middle cranial fossa are 1.7, 3.9, and 10.8 years, respectively. The authors suggested that these differences in the timing of bone maturation may contribute to the fact that acute mastoiditis spreads laterally in infants and medially in older children. [5]
Normal Anatomy of the Middle Ear
The temporal bone houses and is surrounded by many vital structures. The temporal bone is actually composed of four bones, consisting of the squamous, petrous, tympanic, and mastoid segments.
The bony framework of the temporal bone contains multiple air spaces. The most complex of these spaces is the middle ear cavity, or tympanum. The middle ear space is shaped somewhat in the form of a red blood cell stood on end. This space is narrow in a medial-lateral direction and more elongated anteroposteriorly and superoinferiorly.
Laterally, the tympanic membrane, annulus, and the handle of the malleus make up the wall of the tympanum. The inner ear forms the medial wall of the middle ear. The largest anatomic structure of the medial wall is the promontory of the cochlea.
The roof of the middle ear space is formed by the tegmen tympani. This structure separates the middle ear space from the middle cranial fossa. The tegmen slopes inferiorly as it courses laterally along the temporal bone; remember this point during mastoidectomy to avoid violating the tegmen with the drill. In addition, the tegmen is located higher than the superior border of the tympanic membrane, forming a space, the epitympanum. The epitympanum houses the head of the malleus and the body and short process of the incus.
The floor of the middle ear is primarily composed of the bone covering the jugular bulb. The bone over the bulb may be dehiscent, rendering it more susceptible to injury. The floor of the middle ear cavity is located further inferiorly than the lowest extent of the tympanic membrane, creating a space, the hypotympanum.
Anteriorly and inferiorly, the carotid artery limits the tympanum. More superiorly, the eustachian tube, tensor tympani, and cochleariform process can be observed along the anterior margin of the middle ear.
The mastoid air cells lie immediately posterior to the middle ear space. The entrance to the mastoid air cells is the aditus ad antrum. The pyramidal eminence (giving rise to the stapedius tendon) and the incudal fossa can also be observed immediately posterior to the middle ear space.
The middle ear space contains several spaces of clinical significance. The sinus tympani is located between the labyrinthine wall and the pyramidal eminence. This area is a common site for recurrence of cholesteatoma. The facial recess is found between the tympanic annulus and pyramidal eminence. This recess provides improved access to the middle ear space during a tympanomastoidectomy.
Normal Anatomy of the Inner Ear
The inner ear is housed in the bony labyrinth, which is well demonstrated on CT scans. The cochlea lies anteriorly. The cochlea is a conical structure, with its apex pointed anteriorly, inferiorly, and laterally; its base rests near the internal auditory canal and extends outward for 2.5-2.75 turns. Immediately anterior to the cochlea is the carotid artery. The round window is located in the scala tympani of the basal turn of the cochlea. The round window niche houses the round window. This window is the termination of the scala tympani of the cochlea. The niche protects the round window from direct exposure to sound waves in the event of a tympanic membrane perforation.
The vestibule lies posterior to the cochlea, abutting the internal auditory canal medially. The stapes footplate transmits vibrations to the vestibule at the oval window. The 3 semicircular canals emanate from the vestibule. The lateral canal lies 30° from horizontal. The 3 canals lie at right angles to each other.
The endolymphatic sac is posteromedial to the semicircular canals on the posterior margin of the petrous bone. The seventh and eighth cranial nerves (CN VII and CN VIII) course through the internal auditory canal. CN VIII enters the structures of the inner ear to innervate them and CN VII passes laterally and anteriorly to the geniculate ganglion, then posteriorly along the medial wall of the tympanum before heading inferiorly to the stylomastoid foramen.
A retrospective CT-scan study by Saxby et al found the rate of semicircular canal dehiscence in pediatric patients to be significantly lower than rates found in previous studies. The study involved 334 children (649 temporal bones), with temporal bone imaging revealing superior canal dehiscence in 3.3% of patients (1.7% of temporal bones) and posterior canal dehiscence in 2.1% of patients (1.2% of temporal bones). [6]
A study by Tada et al reported that low-dose, 320-row temporal bone CT scanning in children up to age 5 years produced diagnostic-quality images of the middle and inner ear, despite the results featuring more image noise than standard-dose CT scans. [7]
A study by Waldeck et al indicated that in CT scanning–based measurement of cochlear duct length (CDL), as determined for non-malformed cochleae, three-dimensional (3-D) curved multiplanar reconstruction (cMPR) is more accurate than either 2-D cMPR or length estimation based on the diameter of the cochlea’s basal turn. The report also found evidence that with its higher spatial resolution, cone-beam CT can more accurately measure CDL than can regular CT. [8]
Axial CT Images of the Temporal Bone
The images of the temporal bone are examined in 2 planes, axial and coronal, because both views are crucial to an adequate study. The images below are axial sections through a left temporal bone. The images are ordered from the most superior (the first image) to the most inferior (the ninth image).
CT scan, temporal bone. An axial view through the superior portion of the temporal bone, which demonstrates the anterior (a) and posterior (b) crura of the superior semicircular canal. The surrounding otic capsule is observed as dense white bone. The mastoid air cells (c) are lateral to the otic capsule. The squamous air cells are separated from the petrous air cells by the Koerner septum (d). The posterior margin of the temporal bone, or cerebellar plate, (e) forms the anterior margin of the posterior cranial fossa.
 CT scan, temporal bone. The anterior limb of the superior semicircular canal can be observed (a). Posteriorly, the posterior limb of the superior semicircular canal forms the crus commune (b) by joining with the posterior semicircular canal (c). The mastoid air cells (d) and cerebellar plate again are visible.
CT scan, temporal bone. The anterior limb of the superior semicircular canal can be observed (a). Posteriorly, the posterior limb of the superior semicircular canal forms the crus commune (b) by joining with the posterior semicircular canal (c). The mastoid air cells (d) and cerebellar plate again are visible.
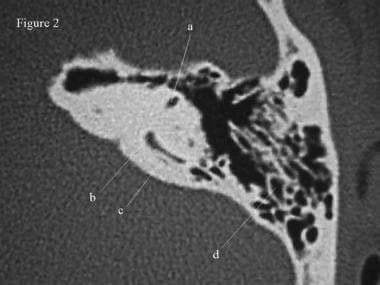
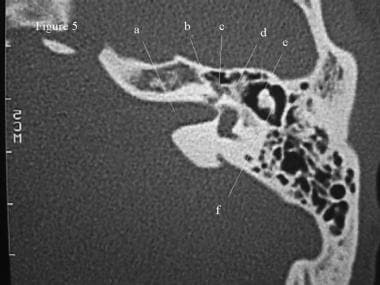
 CT scan, temporal bone. The sigmoid sinus indents the cerebellar plate posteriorly (a). More inferiorly, the sigmoid sinus forms the origin of the internal jugular vein inferiorly. The vestibular aqueduct (b) courses posterior to the posterior semicircular canal (c) and the more anteriorly located superior semicircular canal (d). The superior aspect of the lateral semicircular canal (e) is located lateral to the other semicircular canals. The most superior portion of the internal auditory canal (f), carrying the facial, cochlear, and superior and inferior vestibular nerves, is the lucency in the medial of the petrous bone.
CT scan, temporal bone. The sigmoid sinus indents the cerebellar plate posteriorly (a). More inferiorly, the sigmoid sinus forms the origin of the internal jugular vein inferiorly. The vestibular aqueduct (b) courses posterior to the posterior semicircular canal (c) and the more anteriorly located superior semicircular canal (d). The superior aspect of the lateral semicircular canal (e) is located lateral to the other semicircular canals. The most superior portion of the internal auditory canal (f), carrying the facial, cochlear, and superior and inferior vestibular nerves, is the lucency in the medial of the petrous bone.
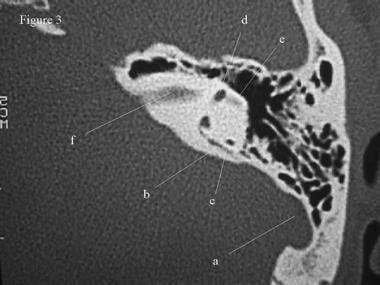
 CT scan, temporal bone. An axial section through the vestibule (a) and lateral semicircular canal (b). The posterior semicircular canal (c) and vestibular aqueduct (d) still are visible posteriorly. The vestibular aqueduct is passing from the endolymphatic sac (e), which indents the posterior margin of the petrous bone, towards the vestibule. Posteriorly and laterally, the sigmoid sinus (f) is visible, and medially, the internal auditory canal (g) is the indentation on the medial border of the petrous bone. Note the middle ear space superior to the uppermost aspect of the tympanic membrane, the epitympanum, which houses the head of the malleus, as well as the body and short process of the incus (h). The petrous apex is visible (i).
CT scan, temporal bone. An axial section through the vestibule (a) and lateral semicircular canal (b). The posterior semicircular canal (c) and vestibular aqueduct (d) still are visible posteriorly. The vestibular aqueduct is passing from the endolymphatic sac (e), which indents the posterior margin of the petrous bone, towards the vestibule. Posteriorly and laterally, the sigmoid sinus (f) is visible, and medially, the internal auditory canal (g) is the indentation on the medial border of the petrous bone. Note the middle ear space superior to the uppermost aspect of the tympanic membrane, the epitympanum, which houses the head of the malleus, as well as the body and short process of the incus (h). The petrous apex is visible (i).
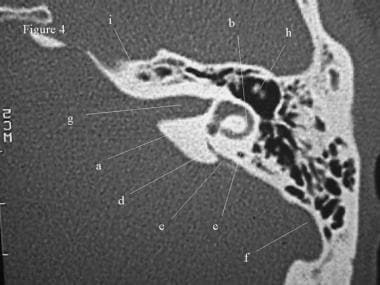
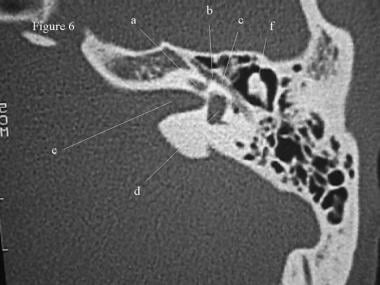
 CT scan, temporal bone. The facial nerve can be observed coursing from the internal auditory canal (a). From here, the facial nerve turns anteriorly as the labyrinthine segment (b). This segment ends at the geniculate ganglion anteriorly (c). The nerve then continues posteriorly as the tympanic segment (d). The section passes through the vestibule, horizontal semicircular canal, and posterior semicircular canal. In addition, the image better depicts the head of the malleus (e) and the incus (f).
CT scan, temporal bone. The facial nerve can be observed coursing from the internal auditory canal (a). From here, the facial nerve turns anteriorly as the labyrinthine segment (b). This segment ends at the geniculate ganglion anteriorly (c). The nerve then continues posteriorly as the tympanic segment (d). The section passes through the vestibule, horizontal semicircular canal, and posterior semicircular canal. In addition, the image better depicts the head of the malleus (e) and the incus (f).
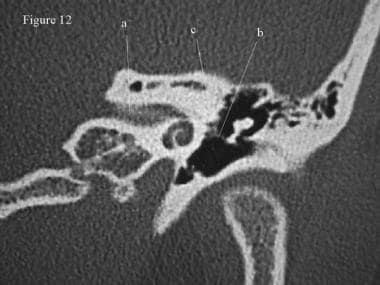
 CT scan, temporal bone. The basal turn of the cochlea (a) is demonstrated. The geniculate ganglion (b) and tympanic branch of the facial nerve (c) also are well visualized. The vestibule (d), internal auditory canal (e), and ossicles (f) are visible.
CT scan, temporal bone. The basal turn of the cochlea (a) is demonstrated. The geniculate ganglion (b) and tympanic branch of the facial nerve (c) also are well visualized. The vestibule (d), internal auditory canal (e), and ossicles (f) are visible.
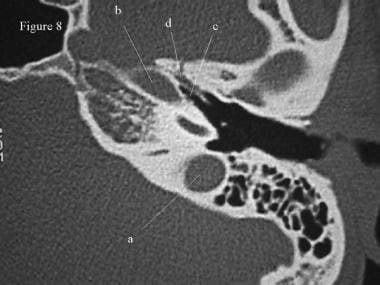
 CT scan, temporal bone. The pyramidal eminence (a), which gives rise to the stapedius tendon, is shown. The space between the medial wall of the tympanum and the pyramidal eminence is the sinus tympani. The external auditory canal (b) and the tympanic membrane (c) are located laterally. The tensor tympani, which runs along the eustachian tube and attaches to the neck of the malleus, is visible anteriorly (d). Finally, the round window niche is observed (e).
CT scan, temporal bone. The pyramidal eminence (a), which gives rise to the stapedius tendon, is shown. The space between the medial wall of the tympanum and the pyramidal eminence is the sinus tympani. The external auditory canal (b) and the tympanic membrane (c) are located laterally. The tensor tympani, which runs along the eustachian tube and attaches to the neck of the malleus, is visible anteriorly (d). Finally, the round window niche is observed (e).
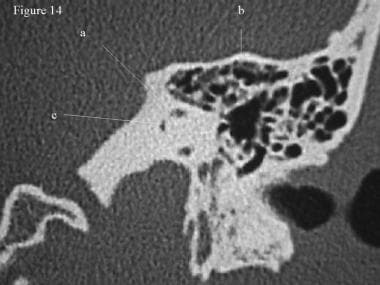
 CT scan, temporal bone. Continuing inferiorly, the superior aspect of the jugular bulb (a) is demonstrated. The carotid artery is located more anteriorly (b). Immediately anterolateral to the course of the carotid is the eustachian tube (c). The tensor tympani muscle shares a wall of the eustachian tube (d).
CT scan, temporal bone. Continuing inferiorly, the superior aspect of the jugular bulb (a) is demonstrated. The carotid artery is located more anteriorly (b). Immediately anterolateral to the course of the carotid is the eustachian tube (c). The tensor tympani muscle shares a wall of the eustachian tube (d).
 CT scan, temporal bone. Some of the inferior-most structures in the temporal bone. The glenoid fossa (a) is observed anteriorly. The carotid artery (b) courses medially and anteriorly. The sigmoid sinuses flow into the jugular vein (c). Anteromedial to the carotid, the sphenoid sinus is observed (d).
CT scan, temporal bone. Some of the inferior-most structures in the temporal bone. The glenoid fossa (a) is observed anteriorly. The carotid artery (b) courses medially and anteriorly. The sigmoid sinuses flow into the jugular vein (c). Anteromedial to the carotid, the sphenoid sinus is observed (d).
Coronal CT Imaging of the Temporal Bone
The images below are coronal sections of the same left temporal bone studied in the axial sections. They are ordered from anteriorly (the first image) to posteriorly (the fifth image).
 CT scan, temporal bone. Coronal section through the anterior temporal bone demonstrates the carotid artery (a) near the basal turn of the cochlea (b). The head of the malleus (c) lies in the epitympanum. The mastoid air cells can be observed superiorly and laterally to the superior margin of the glenoid fossa (d), and the supralabyrinthine air cells (e) can be observed superior to the otic capsule. The middle ear space is separated from the middle cranial fossa (f) by the tegmen tympani (g). To help orientation, note the condyle of the mandible inferior to the glenoid fossa (d).
CT scan, temporal bone. Coronal section through the anterior temporal bone demonstrates the carotid artery (a) near the basal turn of the cochlea (b). The head of the malleus (c) lies in the epitympanum. The mastoid air cells can be observed superiorly and laterally to the superior margin of the glenoid fossa (d), and the supralabyrinthine air cells (e) can be observed superior to the otic capsule. The middle ear space is separated from the middle cranial fossa (f) by the tegmen tympani (g). To help orientation, note the condyle of the mandible inferior to the glenoid fossa (d).
 CT scan, temporal bone. The carotid artery (a) and the cochlea (b) are shown. The labyrinthine (c) and tympanic (d) portions of the facial nerve are visible. The middle ear space extends quite inferiorly, creating the hypotympanum (e). This section passes through the ossicles in the epitympanum.
CT scan, temporal bone. The carotid artery (a) and the cochlea (b) are shown. The labyrinthine (c) and tympanic (d) portions of the facial nerve are visible. The middle ear space extends quite inferiorly, creating the hypotympanum (e). This section passes through the ossicles in the epitympanum.
 CT scan, temporal bone. This section demonstrates the internal auditory canal (a), the tensor tympani muscle (b), and the tympanic portion of the facial nerve (c).
CT scan, temporal bone. This section demonstrates the internal auditory canal (a), the tensor tympani muscle (b), and the tympanic portion of the facial nerve (c).
The first image below provides a view of the facial nerve (a) coursing just inferior to the lateral semicircular canal (b). Another key point in otologic surgery for chronic ear disease is to examine the bone of the lateral canal. Cholesteatoma may erode this bone, increasing the patients' risk of a postoperative fistula. In addition, if the bone of the semicircular canal is eroded, be careful in exposing the facial nerve because the bone over the nerve may be dehiscent as well.
In a study comparing the preoperative findings on high-resolution CT scans (axial and coronal) of the temporal bone with intraoperative findings, Rogha et al concluded that such scans can accurately demonstrate the extent of damage from cholesteatoma. In the report, on 36 patients with cholesteatoma, the investigators found excellent correlation between scan and intraoperative findings for sigmoid plate and scutum erosion and for widening of the aditus, and good correlation for malleus and tegmen erosion. However, scan results correlated poorly with intraoperative findings for erosion of the incus and stapes and for facial nerve dehiscence. [9]
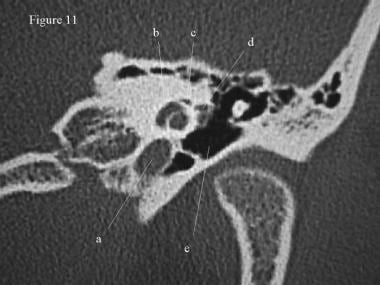
 CT scan, temporal bone. The facial nerve (a) courses just inferior to the lateral semicircular canal (b). The apex of the superior semicircular canal (c) is observed. Laterally, the ossicles are visible (d). The lateral boundary of the epitympanum is the scutum (e), which is a clinically important landmark because erosion of the scutum is often observed in patients with cholesteatoma.
CT scan, temporal bone. The facial nerve (a) courses just inferior to the lateral semicircular canal (b). The apex of the superior semicircular canal (c) is observed. Laterally, the ossicles are visible (d). The lateral boundary of the epitympanum is the scutum (e), which is a clinically important landmark because erosion of the scutum is often observed in patients with cholesteatoma.
 CT scan, temporal bone. This section passes through the posterior semicircular canal (a). The tegmen tympani is well outlined (b). A short segment of the vestibular aqueduct is visible (c).
CT scan, temporal bone. This section passes through the posterior semicircular canal (a). The tegmen tympani is well outlined (b). A short segment of the vestibular aqueduct is visible (c).
Recently, angiographic techniques have been combined with CT imaging to create CT angiography. The resulting images show vascular structures in the context of soft tissue and bony structures. In the temporal bone this is particularly useful for imaging the carotid artery, sigmoid sinus, and internal jugular vein as they course through and along the otic capsule. These images are particularly useful in the diagnosis of venous sinus thrombosis.
Future and Controversies
A study by Lee et al reported that in manual segmentation of cone-beam CT scans of the temporal bone, significant variability was found among reviewers. Manual segmentation of the cochlea, facial nerve, chorda tympani, mid-modiolar (MM) axis, and round window was performed by five reviewers in two sessions, with the Dice similarity coefficient as well as volume similarity, mean Hausdorff distance metrics, and visual review used to determine reviewer variability. While within and across reviewers, the least variability was found for the cochlea and facial nerve, a great amount of variability occurred for the round window, the MM axis, and, especially, the chorda tympani. According to the investigators, “[t]his variability needs to be considered when interpreting the results in studies using one manual reviewer.” [10]
A retrospective study by Szczupak et al indicated that in lower-risk patients, pan-scan CT scanning may be adequate to detect whether temporal bone fractures involve critical structures, without the additional use of dedicated CT scanning. The investigators reported that in the lower-risk group, negative predictive values for pan-scan imaging with regard to involvement of the otic capsule, carotid canal, facial nerve canal, ossicular chain, and tegmen were 1.000, 0.960, 1.000, 0.992, and 0.856, respectively. [11]
Flat-panel detectors in CT scanning have been developed and used in order to obtain higher-resolution images. A 2009 study by Majdani et al compared the imaging of a flat-panel volume CT (fpVCT) with that of a flat-panel digital volume tomography scanner (fpDVT) in temporal bone scanning. The authors found an improvement in image quality, as well as other advantages, among flat-panel detector-equipped scanners; however, when scanning whole cadaveric heads, the differences between these scanners and multisection CT scanners were not significant. [12]
A study by Locketz et al indicated that the fusion of temporal bone CT scanning with PROPELLER (periodically rotated overlapping parallel lines with enhanced reconstruction) diffusion-weighted magnetic resonance imaging (MRI) is superior to PROPELLER diffusion-weighted MRI alone for the preoperative identification and localization of cholesteatomas. The diagnostic sensitivity, positive predictive value, and negative predictive value of the CT/MRI-scan fusion were 0.88, 0.88, and 0.75, respectively, compared with 0.75, 0.86, and 0.60, respectively, for PROPELLER diffusion-weighted MRI by itself. [13]
Similarly, a study by Campos et al found that fusion imaging using high-resolution temporal bone CT scanning without intravenous contrast and PROPELLER diffusion-weighted MRI provided a successful preoperative evaluation of cholesteatoma. In 31 of 33 patients with the disorder, the fused-image results coincided with intraoperative findings, with one false positive and one false negative occurring. [14]
A retrospective study by Zhang et al suggested that preoperative high-resolution CT scanning may be an effective alternative to middle ear exploration for revealing some cases of isolated congenital middle ear malformations. The investigators reported that in most instances, aplasia or dysplasia of the ossicular chain was easily identified via this modality. They cautioned, however, that high-resolution CT scanning is less effective in diagnosing fixation of the ossicular chain, necessitating the use of exploratory tympanotomy. [15]
Questions & Answers
Overview
How prevalent are temporal bone variations on CT scans?
Which areas around the temporal bone have the highest prevalence of pneumatization on CT scans?
What is the anatomy of the middle ear relevant to CT scanning of the temporal bone?
What is the anatomy of the inner ear relative to CT scanning of the temporal bone?
Which findings of dehiscence on CT scans of the temporal bone have been reported?
What is the appearance of the temporal bone on axial CT scans?
What is the appearance of the temporal bone on coronal CT scans?
What is the appearance of the temporal bone on CT angiography?
-
CT scan, temporal bone. An axial view through the superior portion of the temporal bone, which demonstrates the anterior (a) and posterior (b) crura of the superior semicircular canal. The surrounding otic capsule is observed as dense white bone. The mastoid air cells (c) are lateral to the otic capsule. The squamous air cells are separated from the petrous air cells by the Koerner septum (d). The posterior margin of the temporal bone, or cerebellar plate, (e) forms the anterior margin of the posterior cranial fossa.
-
CT scan, temporal bone. The anterior limb of the superior semicircular canal can be observed (a). Posteriorly, the posterior limb of the superior semicircular canal forms the crus commune (b) by joining with the posterior semicircular canal (c). The mastoid air cells (d) and cerebellar plate again are visible.
-
CT scan, temporal bone. The sigmoid sinus indents the cerebellar plate posteriorly (a). More inferiorly, the sigmoid sinus forms the origin of the internal jugular vein inferiorly. The vestibular aqueduct (b) courses posterior to the posterior semicircular canal (c) and the more anteriorly located superior semicircular canal (d). The superior aspect of the lateral semicircular canal (e) is located lateral to the other semicircular canals. The most superior portion of the internal auditory canal (f), carrying the facial, cochlear, and superior and inferior vestibular nerves, is the lucency in the medial of the petrous bone.
-
CT scan, temporal bone. An axial section through the vestibule (a) and lateral semicircular canal (b). The posterior semicircular canal (c) and vestibular aqueduct (d) still are visible posteriorly. The vestibular aqueduct is passing from the endolymphatic sac (e), which indents the posterior margin of the petrous bone, towards the vestibule. Posteriorly and laterally, the sigmoid sinus (f) is visible, and medially, the internal auditory canal (g) is the indentation on the medial border of the petrous bone. Note the middle ear space superior to the uppermost aspect of the tympanic membrane, the epitympanum, which houses the head of the malleus, as well as the body and short process of the incus (h). The petrous apex is visible (i).
-
CT scan, temporal bone. The facial nerve can be observed coursing from the internal auditory canal (a). From here, the facial nerve turns anteriorly as the labyrinthine segment (b). This segment ends at the geniculate ganglion anteriorly (c). The nerve then continues posteriorly as the tympanic segment (d). The section passes through the vestibule, horizontal semicircular canal, and posterior semicircular canal. In addition, the image better depicts the head of the malleus (e) and the incus (f).
-
CT scan, temporal bone. The basal turn of the cochlea (a) is demonstrated. The geniculate ganglion (b) and tympanic branch of the facial nerve (c) also are well visualized. The vestibule (d), internal auditory canal (e), and ossicles (f) are visible.
-
CT scan, temporal bone. The pyramidal eminence (a), which gives rise to the stapedius tendon, is shown. The space between the medial wall of the tympanum and the pyramidal eminence is the sinus tympani. The external auditory canal (b) and the tympanic membrane (c) are located laterally. The tensor tympani, which runs along the eustachian tube and attaches to the neck of the malleus, is visible anteriorly (d). Finally, the round window niche is observed (e).
-
CT scan, temporal bone. Continuing inferiorly, the superior aspect of the jugular bulb (a) is demonstrated. The carotid artery is located more anteriorly (b). Immediately anterolateral to the course of the carotid is the eustachian tube (c). The tensor tympani muscle shares a wall of the eustachian tube (d).
-
CT scan, temporal bone. Some of the inferior-most structures in the temporal bone. The glenoid fossa (a) is observed anteriorly. The carotid artery (b) courses medially and anteriorly. The sigmoid sinuses flow into the jugular vein (c). Anteromedial to the carotid, the sphenoid sinus is observed (d).
-
CT scan, temporal bone. Coronal section through the anterior temporal bone demonstrates the carotid artery (a) near the basal turn of the cochlea (b). The head of the malleus (c) lies in the epitympanum. The mastoid air cells can be observed superiorly and laterally to the superior margin of the glenoid fossa (d), and the supralabyrinthine air cells (e) can be observed superior to the otic capsule. The middle ear space is separated from the middle cranial fossa (f) by the tegmen tympani (g). To help orientation, note the condyle of the mandible inferior to the glenoid fossa (d).
-
CT scan, temporal bone. The carotid artery (a) and the cochlea (b) are shown. The labyrinthine (c) and tympanic (d) portions of the facial nerve are visible. The middle ear space extends quite inferiorly, creating the hypotympanum (e). This section passes through the ossicles in the epitympanum.
-
CT scan, temporal bone. This section demonstrates the internal auditory canal (a), the tensor tympani muscle (b), and the tympanic portion of the facial nerve (c).
-
CT scan, temporal bone. The facial nerve (a) courses just inferior to the lateral semicircular canal (b). The apex of the superior semicircular canal (c) is observed. Laterally, the ossicles are visible (d). The lateral boundary of the epitympanum is the scutum (e), which is a clinically important landmark because erosion of the scutum is often observed in patients with cholesteatoma.
-
CT scan, temporal bone. This section passes through the posterior semicircular canal (a). The tegmen tympani is well outlined (b). A short segment of the vestibular aqueduct is visible (c).
-
Sagittal sinus, bilateral transverse sinuses, and left sigmoid sinus are seen. The right sigmoid sinus is thrombosed and does not fill with contrast. These vascular structures are presented against the background of a 3-D reconstruction of the brain and meninges.
-
Axial CT scan of the temporal bone depicting the round window niche (a).





